Dr. Adrian Baranchuk is a cardiologist and professor based in Kingston, Ontario who has published research and presented on the topic of Lyme carditis at various conferences. He joined Project Lyme to discuss cardiological manifestations of Lyme disease, specifically Lyme Carditis.
Lyme carditis is an infection that occurs when Lyme bacteria enter your heart tissue. The bacteria affect your heart’s electrical system or can cause inflammation (myocarditis or pericarditis). According to a study, 90% of patients with Lyme carditis develop cardiac conduction abnormalities and 60% develop signs of perimyocarditis. 5-10% of cases may also present with fulminant myocarditis, which impacts the heart’s ability to fully contract.
Dr. Baranchuk identifies the following potential symptoms of Lyme Carditis:
Fainting or feeling that you may faint
Dizziness
Chest pain
Palpitations
Perception of skipping beats
Shortness of breath
or Death (very unlikely)
Every time we suspect or confirm Lyme disease, a deeper investigation of whether the cardiovascular system has been affected should be done
Lyme disease is not the only infection that can cause carditis. Indeed, Mayo Clinic recognizes a broad range of viral, bacterial (including Lyme disease), and parasitic infections that can cause myocarditis. While not included in the Mayo Clinic list, tick-borne infections such as Bartonella, Babesia, Ehrlichia, Anaplasma, and Powassan Virus should also be considered as part of the differential diagnosis.
Dr. Baranchuk is exploring research on how vector-borne diseases impact the cardiological system, including a comparison study with Chagas disease. His goal is to further analyze these other infections, as well as patients with persistent infections in order to develop a model for chronic cardiomyopathy. Although the research on co-infections is sparse and relatively new, Dr. Baranchuk’s resolute answer was yes, they can cause cardiological manifestations of the disease.
Before we think in treating, we have to advance the cardiovascular model
Prevalence of Lyme Carditis
Lyme carditis is seen in 4% to 10% of all patients with Lyme borreliosis according to this 2008 study; with another review claiming a range of 1-10%. Dr. Baranchuk agrees with these estimates in terms of identified cases but opines that the actual number is likely higher. Given that not everyone presents with symptoms of Lyme carditis, and these symptoms can be resolved with the antibiotics prescribed for standard Lyme cases, there is a percentage of patients who have likely been underdiagnosed. Even if symptoms seemed to resolve, these patients may have received less than optimal treatment for Lyme carditis, which is normally a minimum of three weeks. In addition, given a lack of understanding of Lyme carditis in the medical community and Dr. Baranchuk’s own clinical experience, there is a likelihood of misdiagnosis with practitioners citing alternative cardiological issues.
The CDC estimates that there are approximately 476,000 new cases of Lyme disease each year in the United States, which means there are likely between 4,760 and 47,600 new cases of Lyme carditis each year. While often overlooked by the mainstream medical establishment, Dr. Baranchuk is optimistic about the future. His research team in Canada, as well as others in the United States such as Dr. Aucott’s team at Johns Hopkins, are further exploring a more accurate reporting methodology that will more accurately convey the true prevalence of Lyme carditis.
Identification and Diagnosis
While we all know tick-borne diseases are frequently underdiagnosed, Dr. Baranchuk states that an increase in patient and provider education can lead to a clearer pathway of identification and diagnosis. He advises that any patient experiencing the symptoms described above or has had a known tick bite immediately request an electrocardiogram (ECG) from their doctor to see if their heart has developed any abnormalities. Additional tests such as an echocardiogram or cardiac MRI may also be needed to determine whether a patient has carditis and the extent of cardiac involvement.
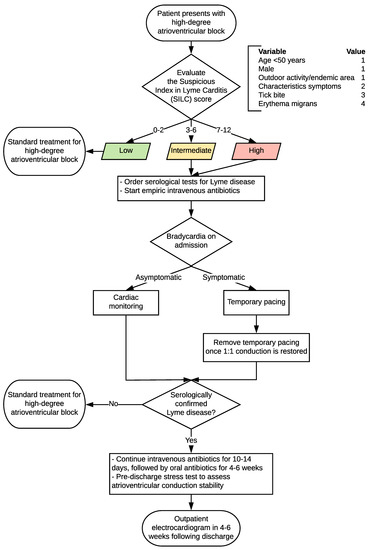
Dr. Baranchuk has also developed a Suspicious Index in Lyme Carditis (SILC) which can be utilized to identify if Lyme disease is the underlying cause of cardiological issues. This diagnostic criterion starts with if the patient has an arterial block and moves down to determine causation and treatment outcomes.
In addition to SILC, Dr. Baranchuk has also developed a method called COSTAR, which is easily adaptable for clinical diagnosis. For each of the acronym letters that apply to you, add a point to your total score. The higher the score, the more likely you are to have Lyme carditis. The acronym refers to:
Constitutional symptoms of Lyme such as fever, malaise, joint pain, and lack of energy.
Outdoor activity in an endemic region.
Sex. If you are male you get a point given they have a higher inclination toward cardiological manifestations (5 to 1).
Tick bite. Not every patient has a known tick bite but if so it highly increases the possibility of diagnosis.
Age. If you are less than 50 and present with cardiological manifestations, then you get a point.
Rash. If you have a shutdown of the electrical system plus rash, it is Lyme carditis until proven otherwise.
Antibiotics are excellent when talking about electrical manifestations of Lyme carditis
Treating Lyme Carditis
Dr. Baranchuk has treated over 20 patients with Lyme carditis. This includes patients who he has diagnosed as well as referrals from other cardiologists. His patients range from those who have just been diagnosed, to those who had already received an implanted permanent pacemaker. He typically treats patients with a standard dose of antibiotics, however, longer treatment courses may be required for presentations such as myocarditis, pericarditis, or dilated cardiomyopathy, especially when there are co-infections in addition to Lyme disease.
According to a study of 105 patients with documented Lyme carditis, 35% of patients required a temporary pacemaker, while only five patients went on to receive a permanent pacemaker. Dr. Baranchuk shared two patient case studies which highlight why it is important to receive an early diagnosis.
One patient case was a 17-year-old who had received a temporary pacemaker. Prior to implanting a permanent pacemaker, Dr. Baranchuk discovered the patient was presenting with signs of Lyme disease. After receiving informed consent from the patient, Dr. Baranchuk initiated a course of intravenous antibiotics before implanting the permanent pacemaker. After one day of IV antibiotics, his patient had retrograded from a high degree to a middle degree block. After five days, he was able to remove the temporary pacemaker, leaving him on a monitor. After seven days, his patient was able to get on a treadmill and the heart was able to beat at its normal rate. Dr. Baranchuk has observed the patient for two years and he remains in complete remission.
Dr. Baranchuk provided another example of a patient who was experiencing a high-degree block. The patient’s physician ordered various blood tests and referred him for a permanent pacemaker. Five days after receiving the implant, the patient was diagnosed with Lyme disease based on serological testing as well as his clinical presentation. Several months later, this patient moved to Dr. Baranchuk’s region and received a referral to see him. Dr. Baranchuk prescribed a course of antibiotics and began to monitor the use of the pacemaker. In the first five days, the patient usage moved down from 95% to 75%. After the three weeks of antibiotics, he was then only using it 1% of the time. Because it had been less than one year since the implant, the pacemaker could be removed without a highly advanced procedure. Given the success of antibiotic treatment, the patient agreed for Dr. Baranchuk to remove it and now lives without a pacemaker.
To conclude, further education and research are needed to ensure that patients are more timely diagnosed and treated for underlying infections such as Lyme. The vast majority of published literature focuses on acute cases with a resolution of symptoms after weeks of antibiotics. There is little guidance for patients who are not timely diagnosed with Lyme disease, who also have co-infections, or who may have reactivated viruses due to immunosuppression. While there is no one size fits all treatment approach, it is important to diagnose and treat Lyme early to reduce the risk of disseminated infection and related complications. If you have Lyme and are experiencing symptoms consistent with Lyme Carditis, it would be prudent to include a cardiologist as a part of your medical team.